Previous Page | Print this page
The Normal Ear Please on the following links to visit an area of interest: Hearing Aids
Links for this page

- External ear canal
- Bat ears
- External ear infections: otitis externa
- Surfer's Ear
- The middle ear
- Glue ear: serous otitis media
- Treatment of glue ear
- Grommet tubes
- Otitis media: infections of the middle ear
- Perforations of the eardrum
- Mastoids and surgery
- Otosclerosis
- Treatment
There are 5 special senses as described in classic Greek Mythology. Sight, sound, touch, taste and smell. Each play a vital role in enabling us to not only function but enjoy the daily stimuli and challenges of life. To be deprived of any one of these causes a significant loss of life quality.
Whereas there’s not doubt that the most dramatic of these special senses is sight if one poses the question “would you rather be completely blind or completely deaf” this raises a very difficult choice. To be blind means a massive dependence on others with a great challenge to one’s independence.
Yet, if one was to consider being completely deaf, that too poses an enormous challenge due to the hearing impaired person being very largely cut off from the normal personal and social interaction of daily life.
Not only does a severely hearing impaired person become socially disadvantaged but they withdraw from society and often lose confidence with provocative changes in personality.
So let’s look at the ear and hearing taking you through not only the anatomy but also discussing how hearing works and the various conditions which can and do affect hearing and what help can be offered.
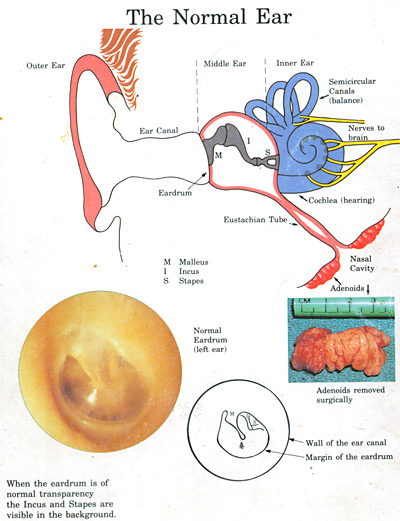
In discussing the ear we’ll divide it into 3 sectors.External, middle and inner.
The external ear is called the Pinna. It forms from a series of mounds which coalesce to form the Pinna producing a classic shape which in itself is important in picking up and transmitting sounds to first the middle and then the inner ear and brain.Whereas few of us retain the ability to “wiggle” our ears. We’ve all seen this in animals where external ear mobility in identifying sounds is still retained.
So let’s look at some fairly common conditions affecting the external ear.
 How wax forms. It differs in different races |
 |
|---|---|
WAX
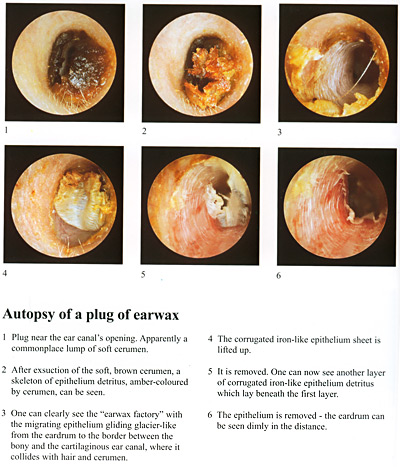
There's nothing dirty about wax. In fact it's an important substance. It lubricates, has antibacterial and antiviral qualities and can be an important factor in protecting the integrity of the ear canal. It's formed by skin peeling off the eardrum and migrating outwards and then meeting the sweat and oil glands secretion.
The combination is what we call wax. If you look at the illustration and you'll get the picture. But wax can cause obstruction and its removal can be problematic unless you have a microscope and a sucker. Something the ENTs all have. Syringing can be extremely difficult for both patient and the Doctor, especially if the wax obstruction is significant. The ENT group tend to use a sucker, the sound of this is quite loud, but the patient needs be reassured.
Once the wax has been removed, only then can you see the appearance of the eardrum. But recall there's nothing dirty about wax. It's significant racial variations. For example the Japanese produce little flakes of skin. A comment on the wax candle. This is a total con. If you like smoke and fire it's fine.
But one regularly sees patients who have damage to the ear by burns or even perforations of the eardrum. It might create a cosy atmosphere after a New Years Eve party... but it's not recommended.

This is a condition which is inherited and runs strongly in some families. In fact when I see a patient with Bat Ears, in literally every case you’ll find either a parent or grand-parent with the same condition.
There are various degrees of Bat Ears but in the most common form there’s a lack of certain cartilage folds in the external ear causing the ears to stand out, some times to such a degree that enormous embarrassment is caused.
It’s a condition which in most cases is easily correctable by an out-patient procedure called Otoplasty where new folds are formed allowing the ear to be repositioned in a much more natural manner. The success rate is extremely high with minimal complications and it is indeed exceedingly seldom that one needs to revise the surgery.
Bat Ears can and do cause enormous embarrassment.Children at school can be mercilessly teased and of course for the teenager, with emphasis on body image, there’s matching embarrassment.
The sad thing is that many parents and often family doctors don’t appreciate the negative impact this can have on a developing personality and the fact that in the vast majority of cases correction can be done, as mentioned, as an out-patient day procedure.
There are various techniques but the one we use removes no tissue from the ear relying solely on a re-fashioning and re-positioning of the natural external ear cartilage.
So recall that Bat Ear deformities can cause significant psychological problems and can often be easily corrected. In adults there is the option of the correction being done under local anaesthesia.
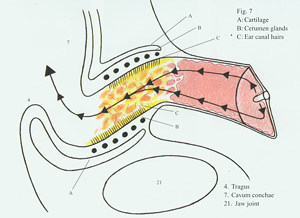
The canal leading from the Pinna to the Ear Drum is important not only as regards its shape being a factor in conducting the sound waves to the ear drum, but also in that it’s rich collection of cerumen producing glands can be a factor in the production and collection of wax which can produce canal blockage. But please recall there’s nothing dirty about wax. It’s a natural product not only lubricating the external ear but also reducing chances of infection.
Remember also the external ear is in essence self-cleansing and that, in the bulk of cases, the ear needs “no help” in keeping itself clean. As regards cotton buds, my usual comment to patients is “if you like your pharmacy’s profit margins and enjoy the sensation of cleaning your ears with a bud…then go ahead. But it really usually does nothing for your ear. In fact you can often push wax deeper in.”
EXTERNAL EAR INFECTIONS: OTITIS EXTERNA
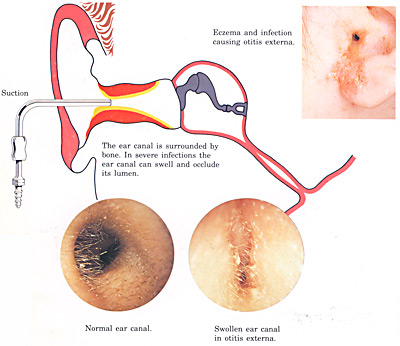
This is a common and very painful condition of the outer ear. The ear becomes inflamed and enormous pressure builds up between the skin and the underlying cartilage with the canal literally being occluded by the swelling and with touching of the outer ear producing significant pain. In many ways one can regard it as an infected eczema.
In most cases it is reasonably easily controlled by cleaning the ear with microscope and suction and application of creams or dressings but in very difficult cases there is surgery available where the canal is widened and this can produce a significant improvement in reducing the occurrence. It has a tendency to recur.
With the enormous popularity of surfing in South Africa this is a condition one is seeing with increasing frequency. What happens is that, due to cold water exposure, overgrowths of bone occurs in the external ear canal. If these become large, and they’re usually multiple, recurrent infections and obstruction and deafness can occur.
 |
 |
|---|---|
| This is what they look like; do something about it! | |
If the surfers were to protect their ears with plugs and hoods there would be significant reduction in osteomata, but of course when you’re young and “body beautiful” and enjoying fantastic surfing, one understands why many young surfers prefer to “take their chance”.
Walking along a beach with many surfers you’ll often, when they come out of the water, see them shaking their heads, rather like a frustrated dog, trying to clear the ear because of water trapped behind the osteomata.
When osteomata cause significant symptoms they can be removed by a surgical procedure where the osteomata are drilled away re-fashioning the canal and reducing the chance of obstruction. Yes there is a possibility they can re-grow and revision surgery may be needed but this is very unusual.
There’s an enormous amount of misinformation about this procedure in the surfing fraternity who imagine it’s complex and full of complication but this is not so. It certainly can take time to do but the procedure is neither dangerous nor painful and has a very high success rate if done by an ENT Surgeon with experience and expertise in this field.
We in Cape Town see it often so for us it’s not an unusual procedure. That’s not to say every osteomata needs surgery. Certainly not. It’s the exception. The results are good.
ARTICLES TO READ:


What do bony surfer's ear and HIV have in common - See Wavescape Article Protect your Ears
The painful Surfer's ear - see Wavescape Article Surfer's Ear
Adrian Waterman Tregoning writes on "Watersports and Your Ears"
Read the full article here.
|
|
|---|---|
| This is what they look like; do something about it! | |
The middle ear comprises the eardrum and the 3 hearing bones – the malleus, incus and stapes. As sound waves hit the eardrum it vibrates and, due to an incredibly complex sequence of transmission, sound is transferred from the stapes (the stirrup bone) to the inner ear and then the brain.
The middle ear is air filled but with a lining of mucus membrane so mucus is produced and this drains from the ear via the eustachian tube to just behind your nose.
The ear and the nose are intimately linked and the linings very similar. And that’s why when you get a cold the eustachian tube, which drains the middle ear to behind your nose and which has a very small diameter, easily blocks causing the sensation of deafness which will usually resolve as your cold disappears.
There are cases where fluid collects in the middle ear and this again will usually resolve but on occasion will need be drained surgically. A minor, local anaesthetic procedure.
So let’s look at some common conditions affecting the middle ear. And lets start with children.
GLUE EAR: SEROUS OTITIS MEDIA
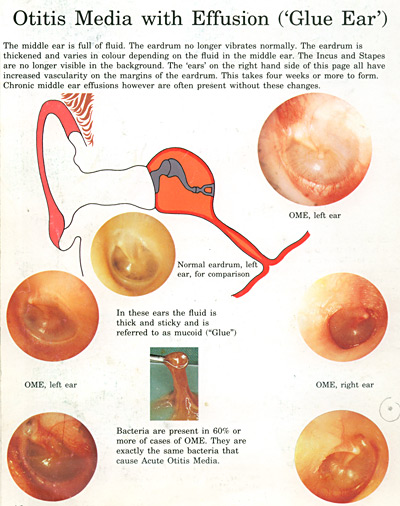
This is an enormously common problem affecting particularly the young child. What happens is that mucus fluid collects behind the eardrum because of inability of the eustachian tube to drain this fluid away. Recall the lining of the ear is made of mucus membrane which means mucus is always produced as a lubricant.
So when this mucus can’t drain away….rather like an overflow pipe being blocked….it collects and reduces the ability of the eardrum to vibrate and transmit sound to the inner ear.
It’s seen particularly in the younger group of children but can occur in all ages.It often happens in winter with all the upper respiratory infections and also in those with nasal allergies. The symptoms can be insidious in that the hearing loss it produces is not noticed. But in more extreme cases up to 40% of hearing can be temporarily lost because of very thick tenacious mucus.
In many it resolves spontaneously but one issues a severe word of warning that unless the doctor you’re seeing understands ears and is able to appreciate and recognise the complications which can occur in mis-diagnosed glue ear, long term and permanent problems can occur with little hope of them being satisfactorily resolved.
Children with glue ear are much more susceptible to infections because of the pool of mucus trapped providing a wonderful culture medium for bacteria entering the ear via the eustachian tube opening up behind the nose.
SYMPTOMS
Common symptoms drawing ones attention to the condition are recurrent ear infections, suspicion that there is a hearing problem and then quite commonly the child being irritable.
One very often finds that if a child requires grommet tubes to resolve the hearing and infection problem the parents will very often say this is now “a much nicer child and far less irritable” after the tubes have been inserted and the mucus drained away.
And as regards the “irritability factor” I see a child every year doing what one calls “the rounds”. The child is irritable, just not behaving normally and provoking people, and what has been missed is glue ear.
Successfully resolving the problem then produces a literal miracle. So what one is saying is that glue ear is very important, is easily mis-diagnosed and needs be carefully followed up if complications are to be avoided.
COMPLICATIONS
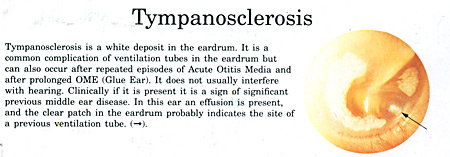
The complications one refers to in particular are that in a chronic mal-treated glue ear because of the eustachian tube not equalising middle ear pressure the eardrum becomes drawn in, severely thinned and permanent damage can occur to, in particular, the second hearing bone which can be badly damaged by “retraction” of the eardrum which has occurred.
These are very difficult cases to help resolve and are often the result of misdiagnosis and mis-assessment. The eardrum can also become permanently damaged.
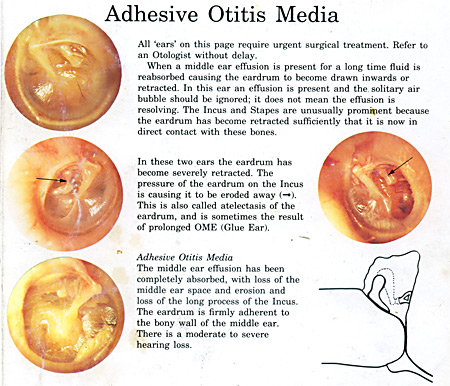
Another complication of misdiagnosed chronic middle ear problems occurring from glue ear is formation of cholesteotoma. This in essence an “invasion” of the middle ear by skin from the external ear migrating through the eardrum and often into the mastoid cells behind the ear.
This is a serious condition and will need surgery. So beware the chronic secretory otitis media with retraction.
Up to 70% of normal glue ear cases are said resolve spontaneously without any medical treatment. We know there are always bacteria in the “glue” but treating this with anti-biotic will not help.
What we sometimes do in conservative treatment is to give a course of oral cortisone, and let me reassure parents that, used in the correct regime, oral cortisones are a wonderful treatment and can produce spectacularly good results.
Don’t be frightened if your doctor suggests an oral cortisone for a short period . It can result in a wonderfully beneficial effect with no small print attached.
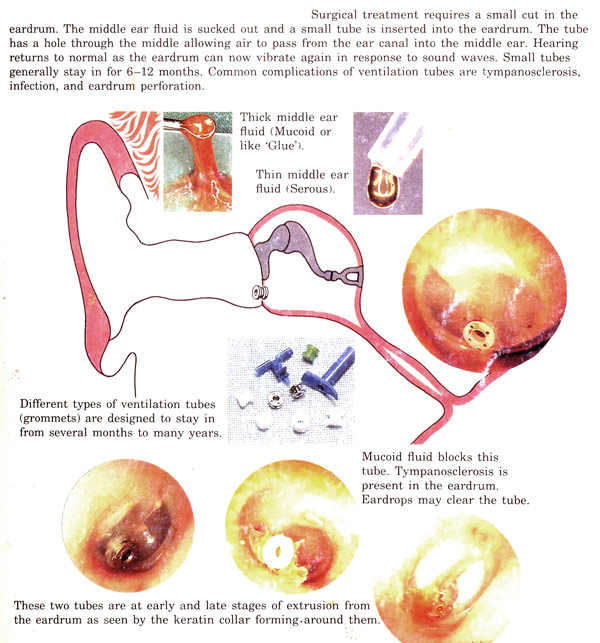
If glue ear doesn’t resolve we come to the topic of “grommet tubes”. In essence what one is saying is “this ear is not going to drain the mucus away, it’s persisting and causing symptoms and we need to do something about that”.
As there is in essence nothing we can do to really improve eustachian tube function what one does is bypass eustachian tube by inserting a grommet tube. This involves making a small incision through the eardrum and inserting the grommet after aspirating the mucus from the middle ear.
There are many different types of grommet tubes but in essence one divides them into short, medium and long term. Should your child require grommets, your ENT Surgeon will discuss which type of tube is to be used.
The average tube will last 6 months whereas the long-term tubes can last a number of years. In essence it’s a wonderfully successful procedure if done for the correct reasons.And one stresses that certainly not every child with glue ear requires grommets. To the contrary.
The procedure’s done on an out-patient basis and in adults under local anaesthesia in the consulting rooms. It has an enormous success rate and because of grommet tubes we, as Ear Surgeons, are seeing increasingly less cases which require major reconstructive ear surgery nowadays.
COMPLICATIONS
Are there possible complications? As with all operations the answer is “yes”. But happily very few. There can be cases where a foreign body reaction occurs to the tube and in this case the ear can be unstable and discharge or quite often bleed. It’s usually easily resolved with local treatment but there are occasions when one will need remove the tube.
This can be done in the rooms not involving the expense of going to the operating theatre. And we all know how expensive they are.
Should there be middle ear infection despite the grommet, this is usually easily treated by topical eardrops. These need to be pumped through the grommet into the middle ear and in most cases this settles the infection.
Once the tube comes out, which it does pontaneously, the eardrum closes and it’s only in the rare exceptions that a permanent perforation can be left. This might especially occur in children who’ve needed repeated grommets.It’s a rare occurrence.
And as regards swimming, the bulk of children with grommets can swim without any protection. If your child is the exception protective measures can be discussed.
OTITIS MEDIA: INFECTIONS OF THE MIDDLE EAR

It’s most unusual for young children not to have intermittent middle ear infections. This is due to bacteria or viruses entering the ear through the back of the nose and entering the eustachian tube to the middle ear.
This occurs particularly in winter with all the winter nose infections.What happens is that fluid or pus is trapped behind the eardrum and, if pressure builds up, this can cause considerable pain.
The pressure may be such that the eardrum actually bursts and the pus released and with this the pain often dramatically subsides. So recall if your child gets a middle ear infection and the eardrum perforates it’s not a “train smash” at all.
It’s nature’s way of releasing the pressure. Not that you wish this to occur frequently. If that does happen you could end up with either a weakened eardrum or a permanent perforation that might need to be surgically closed.
It’s worth considering the naturally history of otitis media in that many will resolve spontaneously needing only pain killers.So don’t think every otitis media needs an antibiotic. They don’t.
In fact there are some interesting surveys questioning whether an antibiotic really does change the natural history of otitis media. Medicine is filled with controversial topics.
But in essence one suggests that, in a severe case of otitis media, antibiotic is certainly useful and many of us will use it earlier rather than later in these cases. One certainly doesn’t want to have ongoing bouts of recurrent otitis media since this can produce scarring not only of the eardrum but also the very sensitive joints around the hearing bones.
So the bottom line will be that for mild cases of otitis media pain killer and decongestants are likely all you’ll need while for the more severe cases an antibiotic and review and possibly drainage and grommet tubes.
It’s very unlikely that middle ear infections in their own right will produce permanent damage to the cochlea….the inner ear.
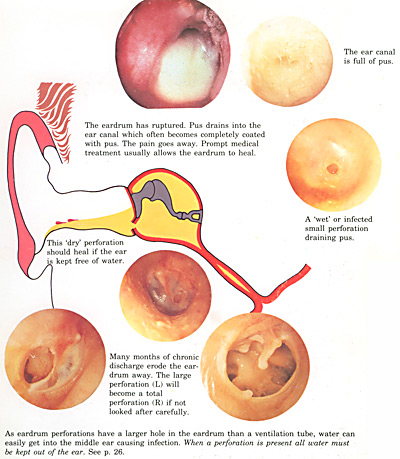
Perforations of the eardrum occur because of a significant number of past bouts of middle ear infection. Although the eardrum is a strong membrane, particularly as regards the middle of its 3 layers, recurrent infections often predispose to by a eustachian tube which is dysfunctional, can cause a permanent hole in the eardrum.
These vary from small to very large.In the case of small perforations there’s quite a high chance that these can heal spontaneously if middle ear infections are kept at bay. Where you have a large perforation there is in fact no chance of a spontaneous closure and surgery needs to be discussed.
The aim of surgery will be to close this perforation, prevent infection coming in from the outside, and in many cases also improving the hearing loss which can occur with the eardrum perforation.
The operation is called a TYMPANOPLASTY.
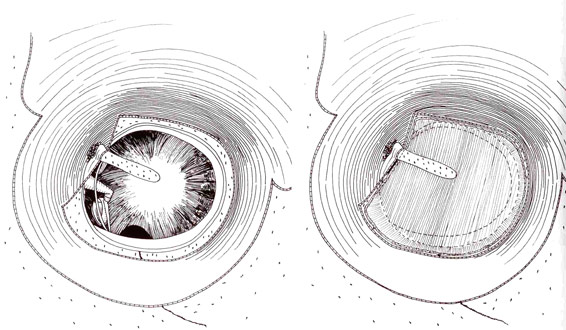
In this operation the lining of the muscle which runs up the side of the skull is used as a graft to repair the perforation. So it’s your own tissue which is used. It’s a delicate procedure but in experienced hands has a very high success rate.
In essence a graft is fashioned from your own tissue to close the perforation and relies on the blood supply of your remaining eardrum and adjacent structures to give it nourishment and allow it to grow.
It’s only in rare occasions that the graft will not pick up sufficient blood supply, break down and need to be redone. The success rate thus in children is particularly high. The operation will include the Surgeon examining the hearing bones to see if they have been affected by the recurrent infections causing the perforation.
In many cases the very delicate joints around the hearing bones will have been affected and thus one can never guarantee that although a new eardrum has been created that the hearing will return to normal. In some cases work has to be done on the hearing bone either at the first or subsequent operation should the hearing loss be bad enough to warrant this.
One needs remember that the eardrum and the 3 hearing bones are all intimately connected and that scarring can occur around these hearing bones affecting their incredibly delicate joints. This is something your Surgeon will discuss with you before the operation.
From the discomfort point of view it’s nice to say that there really is very little pain involved in Tympanoplasty.
Most patients will be able to go home the same day on routine postoperative antibiotics. They are asked to lead a somewhat “controlled” life and not rush around too much as this might affect the healing process of the eardrum.
This of course is very hard to ask young children to do but fortunately because of the excellent blood supply the results are very good for closure.
Leading off the middle ear and behind it is a series of cells forming the mastoid process. These cells can become infected in cases of recurrent middle ear infections producing what is called Mastoiditis. It is always associated with a middle ear infection.
This is a condition which we see rarely nowadays but in the past it was very common for patients to have operations on the mastoid bone. An early Mastoiditis responds well to antibiotics. In severe cases surgery is indicated. One stresses again that this is a rare occurrence nowadays except in our more deprived communities.
This is a condition with a fairly strong family history.In general it occurs more in women than men. It’s due to a change in the otic capsule…that is the part of the ear which involves the nerve and also the stapes (the 3rd hearing bone) which are intimately related.
If the stapes is involved the joint becomes fixed because of new bone formation and the stapes bone is no longer able to move and transmit sound from the eardrum to the inner ear. In these cases a hearing loss of up to 40%, or more, can occur. It usually involves both ears.
As mentioned the condition can also affect the cochlea…the nerve of the inner ear. This cannot be surgically corrected.
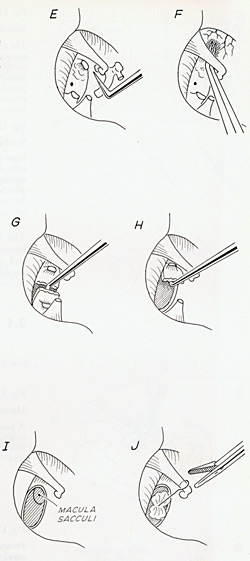
An ear operation: Stapedotomy to replace
the fixed stirrup hearing bone and improve
the hearing.
Where the stapes is involved the patient has options:
- If the hearing isn’t causing too much concern the condition can simply be watched and reviewed on an annual basis.
- If the hearing is causing concern there’s an operation called a stapedectomy where the stirrup, the stapes, is removed and replaced by a titanium prosthesis.
This operation carries a very high success rate. Well over 95% of cases will be helped. There is of course, like in any operation, the small print that there is a small failure rate and cases have been reported where the ear has gone deaf after the operation.
I’ve never seen that. It must be extremely rare. The procedure is literally painless but there’s often some dizziness after the operation. I’ve never seen this persist. In essence a stapedectomy is usually a very successful operation with a delighted patient. It’s delicate microsurgery but in experienced hands the results are good.
- If however the patient isn’t keen on surgery then there’s the option of a hearing aid. Hearing aid technology has improved dramatically, and continues to do so, and it certainly is an option which can be considered providing you’re going to an honest and experienced Audiologist.
In our practice there are 3 Audiologists and we work together as a team which is essential. I’m of the firm opinion that no ENT Surgeon should work without an Audiologist nor should any Audiologist work without an ENT Surgeon in close proximity.
In our case it’s in the same rooms. We have what I regard as the perfect combination.
I’m outnumbered by the ladies so it really is an example of “female power”. Their all being good looking also makes my life a lot easier and more pleasant. But their competence is spectacular and I have nothing but the fullest confidence in what they are doing. This is not something I can say about some other Audiology services.
- The new hearing aids, apart from being very sophisticated, are small and cosmetically acceptable with many options available. The Audiologist will discuss these in full detail.