Previous Page| Print this page
Please click on the below links to visit your area of interest:
Links for this page
- How does the nose work?
- Smell
- The nose and hormones: jacobson’s organ: the sixth sense
- Nasal allergy
- What are the main steps to do if you’re concerned about allergies?
- Medical treatment
- Treatment possibilities
- Antihistamines
- Allergic desensitising
- Diet
- You and your diet
- Surgical treatment for allergic rhinitis
- And on putting it all together
- The sinuses
- The fantasy of clean air
- Sinusitis
- A severe word of warning about some over the counter nasal sprays
- Nasal polyps
- Surgery
- Endoscopic sinus surgery
- Surgery: this explanation is given to all patients before surgery
- The surgical aim
Despite being the most dominating feature of the face, in medical terms the nose, like the ear and throat, could well be referred to as “the forgotten man”. Remember the chat Frank Sinatra has with Bing Crosby in the film High Society and that wonderful phrase : “I have heard amongst this clan you are called the forgotten man.”
It’s appallingly taught at medical school and you can be pretty sure that the average medical practitioner unless he’s a trained ear nose and throat specialist, will have limited ability to examine this vital organ and also understand it. It’s importance is grossly misunderstood. And what is more this lack of understanding by all except the ear nose and throat group means that patients seeking nasal treatment by the non specialist group for significant problems are often misdiagnosed with the potential for inappropriate treatment.
Unless the person examining your nose is able and confident to use the classical headlight…and I don’t mean some vague angle poise lamp… you’re not getting an appropriate assessment. It’s a sad reality that clinics at even the most prestigious academic institutions advertising and providing nasal clinics, often for allergy, are unable to master the use of the headlight, must accept that their patients will suffer the consequences of what we refer to as their “nasal virginity” with patients suffering the consequences of their “ nasal virginity.”
Without the ability to examine the nose, all kinds of pathology is missed and inappropriate diagnosis and treatments suggested. Exceptions to this comment occur for instance in the U.K when non ENT specialists have equipped and trained themselves to offer an appropriate service.
The nose and poorly understood sinuses are intimately linked and their dysfunction causes an enormous amount of poorly recognised disability. There is in fact a well known “ non ear nose and throat specialist” medical professor in America who has for years written about the fact that nasal dysfunction can be an important cause of fatigue and quotes interesting and often persuasive evidence showing that naso sinus surgery has produced impressive results in “fatigue” cases who have sinus dysfunction.
So with all respect to my non ear nose and throat colleagues, unless you have the equipment for examining the nose and mastered examination techniques, you cannot in all honesty claim to offer a competent naso sinus opinion.
Medicine, like life, is full of territorial conflicts and the territory of the nose is no exception.
The nose dominates the face. Its very appearance can often tell you a great deal about its. It’s not only of functional but aesthetic importance and it’s well known in terms of the market place that in job applications if two people have equal qualifications the better looking one will likely get the job. And with the nose dominating the face it’s appearance is a potentially important “employment” factor. So when a patient walks into my consulting room it’s very important I look at the person seeing him in totality and noting with importance the nasal situation.
Very often one sees a patient who despite having no history of breaking the nose, nevertheless has a nasal fracture. Something likely sustained in childhood which was not diagnosed. And this you pick up often by simply looking at the nose externally. Again unless you’re trained in this area subtle changes are going to be missed, and the patient pays the price.
The most prominent feature of the face is the nose. It’s dominant and the shape and structure often tells you a great deal about its owner and personality. Recall Charles de Gaulle. The striking, high-bridged nose in this huge man, told an immediate story about his dominant personality. Many noses can and often do tell a story.
So let’s talk nasal. In evolutionary terms before evolving on land we breathed through fish-like gills whose remnants can still remain and it’s only since becoming land-borne that the nose developed.
It’s structure comprises an intricate composite of bone and cartilage producing a truly amazing organ which is the first physiologic part of the lungs and the only part of the “lung” you can actually see and touch.
Recall we breathe over 20 000 times a day and in doing so inhale some12 000 litres of air which, in today’s modern world, contain a hugely complex and provocative combination of substances. Not only the usual pollens, dusts, fungi and bacteria but the potentially provocative and irritating combinations of our industrial pollution.
It’s asking a lot of the nose to cope with this airborne challenge and in fact it’s often asking too much for it to manage.
If we look inside the nose we see it divided by a mid-line septum. Its sidewalls contain 3 projections called turbinates. These are lined by highly specialised respiratory lining closely linked to the lungs.
In fact they’re 1st cousins and like the lungs their mucous producing cells have a covering layer of tiny arm like cells called cilia which beat the mucus of which your nose and sinuses make over a litre a day….into the back of the nose. Mucus moistens and traps foreign particles.
Cilia are enormously important. They’re like an escalator. If you damage them, such as can occur with smoking, it’s like having pulled off the legs of a centipede. The cilia then move the mucous layer slowly and inefficiently which means the nose is not cleansing itself. The mucus is carried to the back of the nose and swallowed. But remember it’s absolutely normal and goes into your stomach where its digested.
The nose is so efficient that cold air you breathe in is fully warmed and humidified by the time it reaches the back of your nose and fully prepared for the lungs. So in terms of physiologic “foreplay”, the nose is an essential part in preparing air for “consummation” by the lungs and failure in the nasal system to do so carries a potential for secondary lung dysfunction.
Now let’s look at other nasal function, firstly smellthen the incredibly important hormonal function the nose has regards airborne hormones called pheromones and how enormously influential these are.
Smell is one of our most seductive and provocative special senses invading every domain of our lives. It’s mute, almost unspeakable, defying description and challenging imagination providing one with familiar scenes causing memories to rush back. A complex vision leaps out of the “undergrowth.” It opens the door to a kaleidoscope of memories. And when you see the amount of money spent on marketing perfumes, you realise how important smell is, especially in the social context.
But in many ways smell is the “fallen angle” of special senses. Its much underrated and appreciated. On average we can smell some 2 000 different scents. Those highly trained up to 10 000. Not that comparatively we’re well endowed with olfactory cells. Our noses have no more than 6 million situated in an area the size of a postage stamp high up in the nose.
These specialised cells absorb odours and transmit the sensations to the brain. But we compare poorly with, for example, dogs. Sheep dogs have 20 million, Beagles 250 million while in Blood Hounds the olfactory tissue covers the size of a book page…
Those losing their sense of smell are unable to appreciate the wonderful variety of aromas in the air (not that all are wonderful)and lose the ability we all take for granted, to enjoy a meal since with a lack of smell one tastes food only by “texture”. You can’t smell the scent of flowers or perfume and in health situations recognise the smell of bad food. Having no smell can be enormously dangerous.
For example the inability to smell smoke and realise there’s a fire hazard… And then for woman especially, where personal hygiene is a very sensitive issue, the lack of ability to be aware of personal odours is intensely embarrassing. A recent study on those who’ve lost theirsmell, highlighted the fact that it really affects quality of life with many being depressed.
THE NOSE AND HORMONES: JACOBSON’S ORGAN: THE SIXTH SENSE
One of the Greek philosophers divided special senses as follows - sight, sound, touch, smell and taste. But we now add a 6th special sense, namely the ability of the nose to recognise airborne hormones. The pheromones. These are recognised by tiny specialised cells at the base of the nasal septum which interpret the rich combination of airborne and earthbound pheromones carrying essential information influencing social, sexual and territorial behaviour at many levels.
We all throw out a cloud of surrounding pheromones. Advance information as to who and what we are. These are picked up by Jacobson’s organ, the special nerve area at the base of your septum, and interpreted in the brain. For example when you walk into a room and take an instant dislike to someone, it’s likely their pheromones warning you of incompatibility or danger. Similarly recall that in a ladies dormitory at school, the dominant female’s menstrual pattern imprints on all the rest and pick up her menstrual cycle.
In a nursery a mother, in the vast majority of cases, will be able to identify her baby from others by smell and the baby, in the majority of cases, identify the mother from nipple cap odours. When animals lick their babies at birth it’s to produce pheromonal imprinting. If this doesn’t happen, the mother and baby might well lose each other in the herd. These pheromones are unbelievable important and only recently understood. Again it’s the nose which is the home to this special sense.
Pheromones are produced primarily in the groin and peri-anal areas and this is the reason why dogs have that very embarrassing habit of often literally going straight for your groin because of its rich pheromonal production and similarly why they sniff each other so carefully in the peri-anal areas. These are pheromonal production “head quarters.”
To have an allergic nose, which is blocked, runs, causes sneezing and is often combined with itchy, watery eyes and in a significant number of cases, either an irritable allergic cough or asthma of varying degrees is a huge international problem.
It falls into the classic under appreciation scenario of nasal dysfunction, namely it’s being regarded as no more than an irritant not only to the patient but those around can get irritated by the patient’s attempts to make the nose work better.
Nasal allergy is internationally of major concern. It’s incidence is increasing every year due to a complex scenario of reasons and in South Africa it’s estimated that 20% of the population have nasal allergies.
To have a dysfunctional nose, and this comes as no surprise to those who have this problem, can have a significant impact on “quality of life”. Medical surveys now concentrate to a large extent on what impact your medical condition has on your quality of life. And as regards the nose there is an internationally accepted survey stressing that nasal dysfunction has a very significant impact which in many ways matches the problems one has with moderate to severe asthma.
So it’s not something quite literally “to be sniffed at”. And recall again that the nose is the first part of the lungs and that there’s a significant correlation with nasal allergy and asthma. In fact treating a person with a nasal allergy successfully can greatly reduce the asthmatic problems. Regard them in fact as very closely related “first cousins”.
What happens in nasal allergy is that the substance to which you are allergic, be it pollen, dusts, foods, industrial pollution or combination cause an intense swelling of the previously described nasal turbinates which line the side walls of the nose.

The cause of nasal obstruction on allergy
With the rich blood and mucous lining there is release of a substance called histamine which is the corner stone of allergic reactions.
Nasal allergy occurs at all ages. It runs in families so if one or both parents have an allergic background the chances of the child inheriting this are significantly increased. In fact one of the giveaway signs in an allergic family is if the baby is born with eczema that often this is the first sign of allergy which can progress to nasal dysfunction and possible asthma. This is the so-called “allergic march”.
Those with nasal allergies must be assessed by someone with an interest and experience in allergy, especially as there is no quick fix but often a lifetime diagnosis with ensuing health complications and challenges.
WHAT ARE THE MAIN STEPS TO DO IF YOU’RE CONCERNED ABOUT ALLERGIES
- First see someone who has an interest and experience in allergy.
- That person must have the ability to take a detailed history of relevance, be able to understand the nasal anatomy by being able to intelligently use a head light or microscope and know what relevant tests should be done and what medications are appropriate and which are in essence a waste of time.
- Especially in children, going into the diet and environs are important.
- The most common allergens in the air are house dust mite and pollen. Allergy tests identify these and other substances.Tests are either simple skin tests or more sophisticated blood tests.
- Environmental adaptation may need to be considered regarding particularly house dust and of course if animals are a problem. Then control measures, difficult though these might be, need be considered.
- Food Allergy
This depends on the assessment. As mentioned, especially in young children, diet can be a significant factor, whereas in the older group the airborne allergens dominate. There are also a group of some 30% where one simply cannot find the allergen. They fall into the non-allergic group with symptoms identical to the allergic group. The treatment however remains essentially the same.
TREATMENT POSSIBILITIES
STEROID NASAL SPRAYS
The workhorse of symptomatic nasal allergy treatment remains the topical nasal steroid spray. Correctly used they can literally change a patients quality of life for the better and can be used with complete safety over the long term. One can start them literally from the age of 2 years. The spray technique is important and something patients don’t often understand and carry out.
Recall that steroid sprays have no negative impact on the child or adult regards growth patterns and millions of cases have been successfully treated.One stresses this as often the corner stone of symptomatic treatment of allergies. They not only reduce the swelling of the nasal turbinates but also reduce the sneezing and itch symptoms.
ANTIHISTAMINES
Antihistamines are taken by mouth, although there are sprays, and can also be used from a very young age. In many cases they’re very helpful but often need be taken on a long-term basis. One of the side effects, especially in the less sophisticated antihistamines, can be that of drowsiness. Side effects are however relatively rare and the main problem is to accept their need to be taken on a long-term basis which requires discipline.
There are cases where allergy goes into remission in which case treatment can be stopped until the next exacerbation occurs.
The question is often asked as to whether desensitising can offer hope of cure. In certain cases it is a viable option.Particularly in the case of pure house dust mite or pollen allergy. In these a serum can be created which is taken by mouth in a very acceptable form with the desensitising course running over some two years. Whereas it certainly does not offer a guarantee, it’s becoming a very useful option to consider in cases where there is potential for offering a cure to limited allergens.
Just as the air is so widely polluted so we to-day face the fact that many foods too are polluted by chemicals. The food industry is difficult police and are masters at adding many types of chemical preservatives to enhance not only the taste, shelf life but also food appearance.This is particularly so in young children but let us not forget that adults too can have a significant sensitivity to chemical substances and as such questions regarding diet are always an integral part of an allergic assessment.
In our practice this has carefully gone into and if diet seems a potential possibility then they are given the following information on “You and your Diet.”
YOU AND YOUR DIET
The nose and chest are very specialised. The nose warms and humidifies air so by the time it reaches the back of the nose it’s fully warmed and humidified. A remarkable feat. To do this it needs a very rich blood supply to warm and an even richer supply of mucous but the blood supply need not be so rich as the air is already warm. Both have very sensitive linings exposed to air and all the pollutants it may contain.
Our airways may react to a number of different substances in the environment. Common triggers for nasal and chest allergies are house dust mites, tee or grass pollens and cats. Viruses, cigarette smoke and urban air pollution can also aggravate nasal allergies.
However a group of allergy sufferers may have reactions to common goods in their daily diet. (2% to 10% of the population). The foods implicated include milk and dairy products, wheat, citrus, eggs and alcoholic drinks in adults.These people suffer with constant nasal discharges productive coughs with postnasal drip ear infections, sinusitis, bronchitis and sore throats.
Allergy tests may sometimes not identify the cause of the problem and in cases like this, it may be worth, trying a simple empirical exclusion diet to remove a few common food allergens from the diet for 4 WEEKS to see if there is benefit.
The diet should not be used for prolonged periods without consulting a doctor or dietician. An exclusion diet is difficult to stick to, seems boring and you may long for the excluded food but you must persevere as the results may be of great benefit to your health and help reduce your need for medication – good luck and don’t give up!
Two methods are advised:
- Either exclude all 5 foodstuffs (dairy, wheat, egg, citrus and alcohol) for one month, this is advised if symptoms are severe.
- Or exclude each food type one at a time for four weeks until the culprit is identified.
Start with milk
Keep a DIETARY DIARY for the 4-week period documenting all foods eaten and any adverse reactions. Record breakfast, lunch and supper and any snacks between meals. Once the food culprit is identified it’s necessary to reintroduce it into your diet temporarily to confirm you really do react adversely to it.
EXCLUDE DAIRY PRODUCTS
This includes:
COWS MILK, CHEESE, BUTTERMILK, BUTTER, CREAM, ICE CREAM, YOGHURT, MILK CHOCOLATE
Substitutes:
NAN HA infant formula, Soya Milk, Everfresh (UHT long life) milk, Carnation tinned milk diluted 1:1 with water. Cremora may be used as a creamer and can be used to make milk-free ice cream. Kosher “P” foods, Albany chocolate, jelly sweets, goats milk cheese. Lard or Ole margarine may be used as a spread.Ceres apple, grape or pear juices and Rooibos tea are substitute drinks.Others include Nesquick and Creamy Tops (a corn soya drink).Calcium needs to be substituted if milk is excluded for more than a month.
The purpose is to greatly reduce milk protein intake. Everfresh and carnation milk have been through a process which diminishes their allergy potential.
Cremora is similarly affected. Some people occasionally develop an intolerance to soya, but it still is a good substitute for cows milk. Goats milk has a similar protein composition to cows milk and is therefore not encouraged.
EXCLUDE CITRUS FRUIT AND DRINKS
This includes:
Oranges, naartjies, Grapefruit, Lemons, Kumquats.
Substitutes:
Apple, pear, Grape Flavoured Liquifruit, Pick ‘n Pay No Name and Ceres juices. Avoid fizzy cold drinks and those containing sulphur dioxide and sodium benzoate. Dilute the fruit juices for drinking or freeze to make lollipops.
EXCLUDE ALL WHEAT FROM DIET
This includes:
Bread, toast, rolls flour, puffed wheat, biscuits, cakes, cereals, bran, semolina, pizza, pasta, dough, waffles, pancake and gravy which contain wheat.
Substitutes:
Rice, rice cakes, rice crispies, corn, corn flakes, popcorn, mielies, maize cereals, oats, rye bread, barley, potatoes and chips.
Wheat is the most allergenic of the grains and should be completely withdrawn from the diet. Occasionally there may be a cross reaction between wheat, rye and barley. If wheat is excluded for any length of time vitamin B complex should be given as a daily supplement.
EXCLUDE EGGS
Hen’s eggs may be a source of allergic sensitisation and may be worth an empirical exclusion for 4 weeks.
This includes:
Eggs, both egg white and yolk, egg lecithin albumin, ovalbumin, mayonnaise and egg based biscuits, pasta, bread, pancakes, cakes, waffles or deserts.
EXCLUDE ALCOHOLIC DRINKS
This includes:
Wine (white and red), Champagne, Beer, Spirits, Medicines with alcohol.
AND HERE IS AN ICE CREAM RECIPE:
CREMORA ICE CREAM
390 ml Cremora powder
200 ml Boiling water
145 ml Water
35 ml Sugar
5 ml Lemon juice/2.5ml Vinegar
400 ml Frozen concentrate fruit juice (1 tin)
METHOD: Mix Cremora and boiling water. Cool in the fridge. Boil water and sugar till has dissolved. Cool in the fridge. Beat Cremora mixture till somewhat thickened and add syrup, lemon juice and fruit juice gradually while beating. Pour into a container and freeze. Place in fridge 30 minutes before serving
SURGICAL TREATMENT FOR ALLERGIC RHINITIS
IS THERE ANY POSSIBILITY THAT SURGERY CAN HELP?
Yes there certainly is in cases where medical treatment has failed. And this is an area of treatment which is very poorly, or not at all understood, by non Ear, Nose and Throat Surgeons.
- Simple cautery, either with acid or in the case of our practice, with a carbon dioxide laser, can be done under local anaesthesia in the rooms and can often produce a significant improvement lasting at least a year or two. It can easily be repeated.
- Surgical reduction of the turbinates can also be done to improve the airway. This requires a general anaesthesia and an out patient stay in the hospital.
- There are certain cases which respond to injection of cortisone into the actual substance of the turbinates.
This has fallen out of favour for some time but there’s no doubt, that in selected cases, it remains simple treatment done in the rooms which can be very useful.
- Correction of structural abnormalities complicating the medical treatment
AND ON PUTTING IT ALL TOGETHER
Allergic rhinitis is common often producing significant nasal dysfunctional problems. It needs to be intelligently assessed, recalling its relationship to the lungs and asthma and allergic conjunctivitis.
Its treatment requires appropriate examination by a nasal expert, and with diagnosis then having been made, an assessment of treatment options which vary from medical to surgical or a combination.
Allergy is unfortunately often a “ life time diagnosis” and patients need understand the discipline required to accept treatment which is often long-standing and requires patient discipline.
Here’s a controversial topic. To this day we still have a very poor understanding as to exactly what function sinuses play in the modern day environment. In essence we don’t know. Suffice to say they can cause a huge amount of medical difficulty.
There are in essence 4 main sets of sinuses, which lie above, between, and below the eyes and at the back of the nose. All drain into the nose by a highly inefficient drainage system, which easily blocks causing sinus dysfunction.
Being intimately connected to the nose you’ll understand that sinus dysfunction is in many ways secondary to the kind of air we breathe placing an unreasonable demand on the nasal lining and its complex functions.
Clean air is pure fantasy. Most of the air we breathe consists of minute particles of salt, clay, ash, a few viruses in transit between hosts, several bacteria, 50 – 60 fungi and a couple of minute algae and a slew of industrial pollutants and the common respiratory allergens with which we’re “au fait.” We share our planet with permanent aero plankton.
- The cleanest air is over Antarctica, but even that has 200 000 bits and pieces in every lungful.
- Over a 6 lane highway – rush hour Los Angeles – the count rises to 2 million per lungful.
The main sinuses are the frontal lying above the eye, the ethmoids between eye and nose and the maxillary, below the eye. Of these the ethmoid is by far the most important and complex. It contains multiple inter-leading cells draining into the nose and is also the sinus into which both the frontal and maxillary sinuses drain.
It’s thus the absolute cornerstone in terms of sinus dysfunction with both medical and surgical treatment to a large extent, directed towards them.
THE ETHMOIDS ARE THUS THE KEY SINUSES
The definition of what sinusitis actually means still remains very controversial. For many it simply means that they have a “blocked nose” in which case the vast majority of cases are due to nasal allergy or have non-specific reactions in the nasal lining. Both cause the same type of symptoms.
What one in essence is saying is that when a patient comes in saying they have sinusitis, only in the minority of cases is it largely due to a bacterial infection.
You can certainly get secondary bacterial infections due to poor drainage of the sinuses but the bulk of cases are not primarily bacterial. As such one needs to stress that the over-use of antibiotics in so called ‘sinus’ cases is unfortunately widespread and due to a poor lack of understanding of nasal functions.
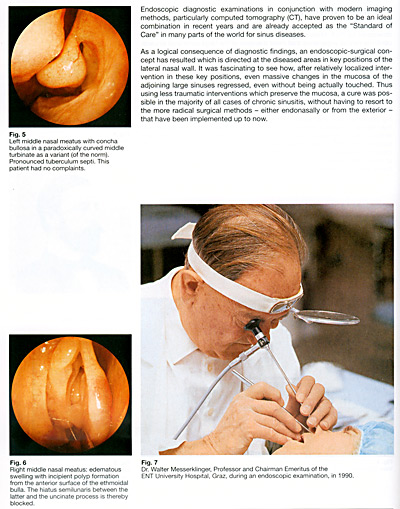
Heinz Stammberger who is an Austrian and one of the most highly respected ENT Surgeons in the world, stresses that determining the importance of various factors is exceedingly difficult.
His group is, in my opinion, the most prestigious and believable group internationally in talking honestly and openly about what can be offered in those cases who have chronic sinusitis where surgery is indicated.
In our practice, once the patient and I have decided that the condition is in fact chronic and will not be resolved by further medical treatment and is causing sufficient symptoms to warrant surgery, the following explanation of what we have agreed on is given to the patient.
A SEVERE WORD OF WARNING ABOUT SOME OVER THE COUNTER NASAL SPRAYS
There are a number of nasal decongestant sprays available over the counter from chemists. These are highly efficient in short term treatment of a blocked nose but if used for longer periods can produce irreversible allergic reactions to the nasal lining. This causes permanent nasal dysfunction with treatment being extremely difficult often needing recourse to surgery.
Be warned. Do not become an addict to these sprays. You’ll heap up a huge amount of problems for yourself and complicate your medical treatment.
NASAL POLYPS
Nasal polyps occur not infrequently causing blockage of the nose, reduction in smell and sinus complications. They’re not due to allergy and we really aren’t certain what causes them, although currently there is a feeling that might well be due to fungi. And as regards fungi, recall that there’s a huge amount of fungus in the air around us : there are in essence 2 tons of fungi for each person in the world.
Polypi usually start in the middle sinus…the ethmoid…but can also involve other sinuses. As they increase in size they cause progressively more symptoms with obstruction and loss of smell. But remember unless your doctor is able to examine the nose, either with the head light or the microscope or endoscopes (the latter two are the most sophisticated) your polypi can and will often be missed.
Not only will polypi be missed but also deviations of the nasal septum which are an additional and not infrequent cause of the “blocked nose.” Treatment of nasal polypi will involve in most cases a limited CT Scan to give accurate assessment of the extent of the polyposis.
All patients with nasal polyps and symptoms need treatment.
- In most cases it’s recommended to start treatment with a nasal steroid spray and if symptoms have disappeared after treatment for a month, the nasal steroid can be continued as the only treatment. This only happens in rare cases.
- Steroids by mouth are enormously effective also often bringing back the sense of smell, albeit unfortunately only temporarily in some cases, and are a vital part of the treatment plan. In essence they’re a life saver in terms of producing a quick result but are not something which one gives for prolonged treatment.
An operation done with either the endoscope or microscope (removing polypi from the sinuses) is often indicated when the above treatment has not been successful. It’s a highly successful part of the treatment plan but needs be done by someone experienced in this field of surgery due to the intricacies of the area of the operation.
One can never get polyps out “by the root” so there’s always possibility of recurrence which is however much reduced if the patient accepts that surgery is part of the treatment plan and that the use of nasal steroid sprays post operatively and on occasion oral steroid, are part of the long term treatment schedule. Combined therapy is very often what the patient is in reality faced with.
Again one stresses that the group most qualified to talk and examine the area is the Ear, Nose and Throat Surgeons. One’s stressed before that without the appropriate understanding and instrumentation, miss-assessment and mis-diagnosis and inappropriate treatment can and will occur.
One sees far too many cases where antibiotics has been given out inappropriately and we all know that taking unnecessary antibiotics can have very negative side-effects.
ENDOSCOPIC SINUS SURGERY:
There’s been a dramatic change in the surgical and medical approach to sinus problems and although we haven’t achieved miracles … those remain as evasive as ever … with the increase in understanding how sinuses work results have significantly improved. We dramatically changed the manner in which surgery is now carried out as well as indications for operations.
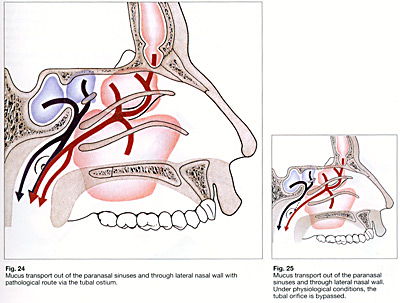
In essence no one knows what the sinus function is. It remains total mystery. But what we do know is that sinuses drain by the most appalling and inadequate systems into the nose and that the main problems are caused by obstruction to this very poorly designed system.
Without going into excessive detail tiny cilia continually beat mucous from the sinuses into the nose. They follow an absolutely fixed pattern in terms of direction and the mucous drains to behind the nose and is then swallowed. So post-nasal discharge is no more than an excess of this mucous of which one is aware.
Often associated with allergy. Of importance to note is that it does not drip into the lungs but is swallowed and digested. It’s usually normal non-infected mucous in most cases. Clearly there are occasions when it can become infected.
We have four pairs of sinuses situated above next to and below the eye as well as further back. They all inter-link by the very poor draining system.
Any obstruction to the drainage passages will cause mucous to stagnate whereafter infection can occur. Nasal polypi can also occur due to a combination of factors which have yet to be fully understood. Suffice to say allergy remains a very significant factor in causing sinus problems and that as always medical treatment remains the corner stone of sinus treatment with surgery only used when this has failed or for other specific indications.
As regards the change in sinus surgery the change has been towards more limited focussed surgery with concentration on removing only diseased tissue and improving the drainage system. By doing this one hopefully achieves better sinus function because more oxygen can get into the sinuses and that means the tissues are able to function more normally.
Clearly though surgery is part of the treatment after the operation medical treatment will in almost all cases continue for prolonged periods.
SURGERY: THIS EXPLANATION IS GIVEN TO ALL PATIENTS BEFORE SURGERY
The operation is under general or local anaesthetics and takes average of 1 – 1½ hours or longer depending on what surgery is necessary.
Surgery is done either by a microscope under magnification or through an endoscope. Both allow detailed visualisation of a very complex area of the body. Recall that not only the eye but the frontal lobe of the brain are close to where the procedure is done. Hence the need for very delicate focussed surgery.
You have discussed the reasons for surgery and asked questions as to why this is necessary and assuming that surgery has been indicated and carried out allow me to comment on the what the post-operative course will usually entail.
HEADACHES
They’re not often troublesome but in certain cases can be present for the first few weeks but are usually well controlled by aftercare procedures and the necessary pain killers. If severe please phone me.
SLIGHT BLEEDING
This is common as well as a mucoid discharge for some days. One suggests you don’t blow your nose too hard the first few weeks.
SWELLING AROUND THE EYES
This is unusual but can take place and is usually related to blowing the nose too hard after procedure. Should this occur it’s usually self-clearing within a few days. If the swelling is severe phone me.
POST-NASAL DRIP
This is common and can carry on for a number of weeks after the procedure. Recall the lining of the nose is built to make mucous and as such following surgery it will have been irritated hence the increase in discharge. It’s advisable to protect the nose from extreme cold and dusty conditions.
SWIMMING
This is encouraged and allowed once you’ve healed. This often takes a month or so. The usual stay in hospital is one night and the amount of sick leave required from 7 – 10 days.
Recall the aim of the operation is to allow better drainage of the sinuses and to allow the sinus linings to come back to as normal as possible. By doing this one decreases the attacks of infection and by allowing more oxygen to the sinuses clearly much benefit is derived.
But one stresses again the medical treatment remains an enormously important factor and patients must realise that surgery is often only part of treatment and not the total answer. Clearly if you have an allergy, this is the lifelong situation and one needs take responsibility for this and appreciate that treatment is ongoing and longstanding.
I hope all goes well with the surgery and hope what you and I have discussed pre-operatively will come to be and that together we’ll be able to control your sinus problem far better than was the case pre-operatively.
It’s absolutely vital for you the patient to understand what one hopes to achieve and all too often one realises that although the patient appears to understand what you’re talking about, they really are just politely agreeing with you and not being fully informed. That’s why we give you the patient this print out in writing.