A HISTORICAL OVERVIEW
Partial or complete loss of a nose causes severe facial disfigurement with tremendous aesthetic and psychological consequences. Many ancient sculptures are examples of this mutilation where the nose has been broken off.
The earliest attempts to reconstruct noses were in India in 1600BC. This was followed by development by the Italians, Americans and in the 18 – 20th Centuries the Germans.
Jacques Joseph is considered the founder of modern rhinoplasty and to distinguish him from three other Professors named Joseph working in Berlin, he was popularly known as “Noseph” to distinguish him from his Gastroenterologic and Dermatalogic colleagues.
PHYLLOGENESIS
Phyllogenetically the necessity of having noses is based on our transition from aquatic to terrestrial life. Originally, as vertebrates, we breathed through gills until becoming land-borne and through evolution the human nose became a highly efficient aerodynamic body with very specialised functions.
Recall how important nasal physiology is. The nose is lined by some 80 000 mucus glands and, having a very rich blood supply, converts cool air into fully warmed humidified air by the time it reaches the back of your nose.
It’s now fully prepared for the lungs. Nasal breathing in physiological terms, is the only acceptable way. Mouth breathing tends to dry out the lower respiratory tract predisposing you to various conditions such as phayrngitis, laryngitis, bronchitis, etc.
The nasal mucosa is a frontline of the human immune defence system and with each breath responds to and defends against a variety of antigens and allergens, bacteria viruses, etc.
Also remember that the nose is the first part of the lungs and the airway is called the “United Airway.” It’s a completely integrated and interdependent unit working in synchrony with nose, throat, voice box and lungs.
Recall that on average most of us can smell some 2 000 – 3 000 different odours whereas those specially trained can quadruple that. The sense of smell is situated high in the nose covering an area no bigger than a postage stamp which relays information to the brain being intimately connected with areas controlling behaviour patterns such as eating, drinking, sexual behaviour, hormonal regulation and emotional perception.
This explains why olfactory stimuli have very rapid and direct access to the deepest centres of human emotions.
As such the interior of the nose is highly specialised separating the air into two streams. The main stream is directed over the lower nasal floor while the smaller upper one, which subsequently divides into 2, reaches up to the olfactory cells.
Not to be forgotten is the fact that the Vomeronasal Organ (Jacobson’s Organ), lying at the base of the nose, is of vital importance interpreting airborne hormones.
This information is transmitted to one of the oldest parts of the brain and influences essential social and mating behaviour having a very significant influence on our lives. We all produce a cloud of airborne pheromones, originating primarily from the peri-anal, perineal and armpit areas giving us a personal and characteristic pheromonal cloud.
For instance a good example of how important they are is when you take an instant “dislike” to a person. It’s very possible the pheromones are warning you “this is not your kind of person.”
Similarly in a nursery both mother and baby are in a high percentage of cases, able to identify each other simply by the odour on nipple caps or blankets. In a female dormitory the dominant female’s menstrual cycle will imprint on all the others because of her pheromonal status.
And when animals lick their babies at birth…this is pheromonal bonding which helps them define each other more easily in the herd. There are many more examples. Lyall Watson’s book “Jacobson’s Organ” gives a superb overview.
So nasal function is enormously complex and sadly misunderstood. As mentioned in the website introduction, that famous comment Bing Crosby makes to Frank Sinatra in the film High Society… “I have heard amongst this clan you are called the forgotten man”… seems very appropriate not only regards the nose but also to the ear and sense of hearing.
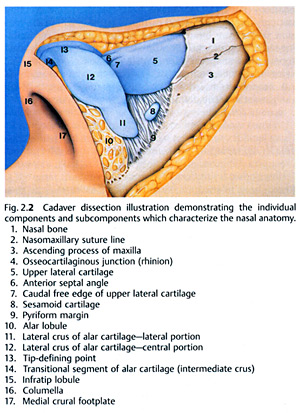
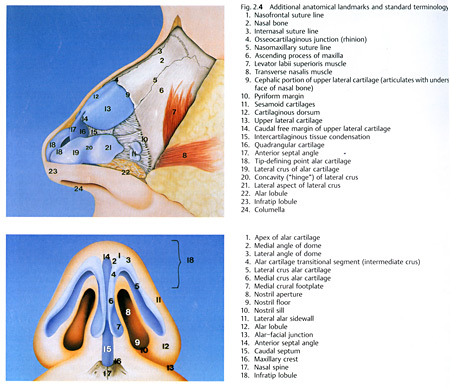
NASAL ANATOMY
SURGERY OF THE NOSE : CORRECTIVE RHINOPLASTY
Although the history of modern rhinoplasty extends back barely one century, the traditional Reduction Rhinoplasty has given way to a nasal reconstruction procedure characterised by careful preservation and re-orientation of tissues.
There’s now very strong emphasis on exacting anatomical analysis with increased understanding of the interplay between various anatomical variants. The creation and preservation of normal airways is vital and this must be balanced with individual aesthetic judgements of surrounding facial features and overall stature.
No single technique will be appropriate for every nose and as such the Nasal Surgeon must be able to call on a wide variety of surgical skills.
The objective of an Aesthetic Rhinoplasty is creating a nose drawing no attention to itself but enhancing the beauty of the eyes, allowing for comfortable nasal function and blending with other facial features. This might seem a simple statement but is extremely complex.
INDICATIONS
Rhinoplasties are done as a result of a patient request to correct perceived anatomical nasal abnormalities and the reasons might include unhappiness with the shape, a poorly functioning nose, abnormalities from previous nasal operations and secondary affects of trauma.
As with all operations there are not only absolute but relative contraindications. Among the absolute are bleeding disorders, pregnancy, systemic illnesses which might be worsened by Rhinoplasty and, most importantly, significant psychiatric disorders….or unrealistic expectations.
SURGICAL TECHNIQUES
Rhinoplasty, as a bilateral and often difficult operation, is one of the most challenging aesthetic facial procedures since no two procedures can ever be the same. Equally importantly the Surgeon is not able to control the healing processes. Every patient’s nasal configuration requires individual and unique planning. So there’s no single technique suitable for everyone.
It’s an operation approached as an anatomical dissection with exposure of structures requiring alteration, with conceptual shaping and repositioning with excision kept to minimum and cartilage grafting employed when needed. There are more problems created from over correction of nasal abnormalities than from conservative correction.
And as always there’s a truism applicable, namely that “it’s not whats removed that’s important but what’s left behind.” In the words of one of the world’s Masters of Rhinoplasty, Eugene Tardy, it’s “millimetre surgery”.
Amongst the most difficult areas to correct is the nasal tip with the need for very careful analysis.
There are various surgical approaches to the nose classified essentially into “closed and open.” Currently there’s a great popularity for the open exposure but there is also concern that because of the wide exposure, a large amount of tissue is exposed which can lead to increased and excessive scarring compromising the results. So each case needs be assessed as to which approach is appropriate in consideration of how the operation is to be done.
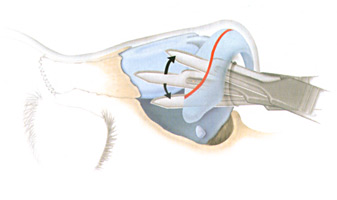
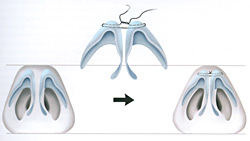
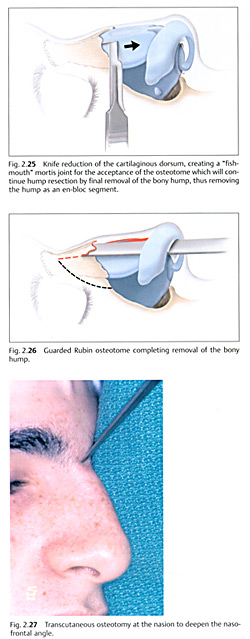
There’s often necessity to modify the elements making up the nasal septum structure, both bone and cartilage as well as reducing and aligning elements of tip cartilage and bony and cartilaginous dorsal humps. Significant use is made of grafting and as always is the preference for the patient’s own tissue. Hence cartilage grafts either from the patients nose or ear are widely used.
AND ON PUTTING IT ALTOGETHER:
Surgery to reconstruct or refashion the nose either for functional or cosmetic reasons is often a difficult and challenging procedure requiring significant experience and expertise. As mentioned no single technique will cover every case and combination techniques are often required. The goal is to provide a nose that is aesthetically pleasing and matchingly functional. This combination can in some cases be difficult to achieve.
It’s also essential cases be followed up. We see our cases on an annual basis to review the situation and there are occasions when, as time goes by, touch up procedures need be done. This is something a patient must understand and accept as an important reality. |