With the nose dominating the face it’s not surprising a fractured nose is one of the most frequent bone fractures of the entire human body. The energy required to cause a nasal fracture is much lower than for other facial bones and more than 50% of all facial fractures are nasal injuries.
With the increase in International trauma, and South Africa is no different one assures you, one sees many more nasal fractures. And the sadness is that in general the complexity and consequences of inappropriate treatment remains widespread. The nasal fractures often occur in association with other major injuries and tend to get lost in the management plan.
Or even worse the patient is simply told “don’t worry, it will heal on its own.” Well of course it will heal on its own. And often produces not only a nose which looks appalling but is also a functional problem.
All this can be avoided if the nose is seen assessed and treated by an Ear, Nose and Throat Specialist. One who has a particular interest and experience in the nose and its management.
So the bottom line is that if there is trauma to the nose, it must be assessed swiftly so that a management plan can be instituted.
TRAUMA – RELEVANT ANATOMY OF THE NOSE
One needs to understand the detailed anatomy of the nose when assessing a nasal fracture. The anatomy is complex and detailed, hence the need for a nasal specialist. Also recall that in severe nasal trauma ligamentous attachments from the eye to the nose can be affected.
The nose, being a central and prominent facial element can function as an absorber of energy and protective buffer of the brain encased in the bony skull. The cartilage portions of the nose have a high level of flexibility helping absorb trauma without permanent damage. Also recall the different results of trauma in older people versus the young.
The older you get the thinner your bones become, hence the easier they fracture, whereas in children “green stick fractures” predominate. Children’s nasal bones are shorter with the larger cartilaginous portion and additional protection is given as the bones are embedded in thicker, softer tissue. The nose is also less prominent than in adults, reducing the trauma consequences as the striking energy is spread across a larger surface.
On the other hand never forget the various anatomical growth zones in the child’s nasal skeleton, which can be strongly influenced particularly with the growth spurt of the teenage years.
ASSESSING NASAL FRACTURES
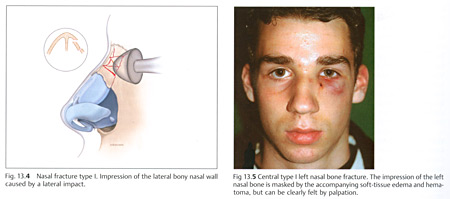
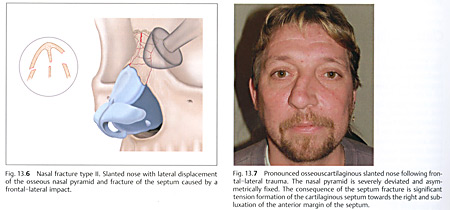
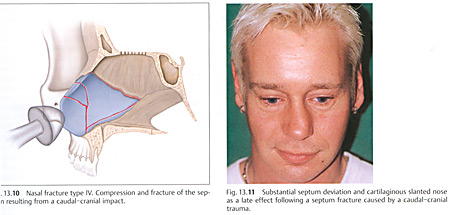
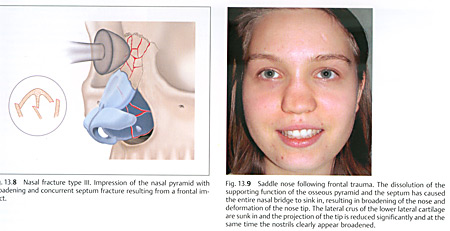
It’s absolutely essential that detailed history is available as to the direction of the force causing the fracture. In essence there are 4 types of fracture depending on the force direction. (Insert pictures of the different type of fractures)
EXAMINATION AND PALPATIONS
The external examination includes inspection of the nose as well as palpation and a detailed examination of the interior nose. Unless these are done the chance of a mis-diagnosis and its consequences are real. Special equipment will be needed such as a headlight, cocaine hydro-chloride to decongest and anaesthetise the interior and special instruments such as a microscope or endoscope to enable intelligent examination.
Without these the assessment is going to be essentially incomplete and a bleed into the nasal septum missed with potentially disastrous consequences regarding collapse of the nasal structure.
X RAYS
This should be written in bold letters in every trauma centre. Namely that the standard X Rays taken of the nose are in essence largely useless and not cost effective. Articles have been written on the broad mismanagement of radiological examination techniques and the diagnoses for management of nasal trauma.
In essence a coronial and possible axial computed tomography would be necessary if you wanted to make a radiological diagnosis. But in essence in most cases one doesn’t need X Rays. It’s the clinical judgement of the Nasal Specialist which is essential and highly cost effective.
MANAGEMENT OF NASAL TRAUMA CHRONOLOGICAL PROCEDURE:
With nasal trauma the question is always raised as to what the best time is for treatment. Very few nasal fractures are treated within the first few hours when the soft tissue swelling is still minimal. If they are seen very soon, then in the case of simple fractures, you can reposition the fractured nasal bones immediately and usually under local anaesthetic.
However most nasal fractures are treated after a longer time interval. With adults the possibility for what we will call “primary treatment”, is limited after a time span of some 2 – 3 weeks and with children within 5 – 7 days. After that the improper fixation of fractured bone and cartilage is to be expected.
In the majority of cases patients come after 5 – 6 hours by which time there’s significant swelling and the assessment of the bony cartilage displacement is more difficult. Once having made your initial assessment, one waits for 3 – 5 days after the trauma before carrying out any repositioning measures. The exception is the septum haematoma (bleeding into the septum) which needs to be drained immediately.
CLOSED REPOSITIONING TECHNIQUES
If the bony fragments are only displaced to the side then one can do what we call a finger manipulation. Obviously in all these manipulation cases local anaesthetic is used.
However if fragments are depressed, then they need to be lifted and repositioned and then one will need a variety of instruments. There is still a possibility that this can be done under local anaesthetic. After the manipulation the nose is stabilised with dressings depending on what damage has been done and the corrective procedures taken.
OPEN REPOSITIONING TECHNIQUE
With the more severe nasal fractures or when there has been a time delay and one can no longer offer the possibility of reduction under local anaesthesia, then a formal reconstructive Functional Rhinoplasty needs to be done.
This is usually under general anaesthesia although local anaesthetic techniques with sedation are possible. In essence the nose is then formally opened by surgery with examination and assessment of where the damage has been done and appropriate corrective and reconstructive techniques carried out.
MANAGEMENT OF NASAL TRAUMA IN CHILDREN
This requires special comment. Although the current extent of trauma may seem relatively minor, the significant function and aesthetic consequential damage is possible and this might only appear at the much later teenage growth spurt time.
Remember there are growth zones particularly in the cartilaginous nasal septum, and as such conservative measures should always be preferred in these cases. One needs to watch and follow up these children and if distortion of the nasal anatomy occurs and reconstructive rhinoplasty is needed, this should ideally be postponed until the end of puberty at the earliest. Ideally around some 18 years.
CONCLUSION
Fractures of the nasal bones are frequent and with the increasing amount of trauma the frequency is increasing significantly. Remembering that the nose dominates the face and is vitally important in ones appearance, it’s a sad reality that in many cases, a fracture of the nose is regarded as something minor, and thus often very poorly assessed and treated.
The consequences can be severe. Namely a nose which is significantly inappropriate for the face, and also functionally deficient, leading to secondary sinus complications. Also remember there is the reality that in everyday life a person with a nose which appears to be broken, is often classified as a “rough person.” And then recall the reality that in a job interview if both candidates are the same the person who is the better looking will likely get the job.
And if you have a broken nose that puts you at a significant disadvantage. So recall from both an aesthetic and functional point of view if you fracture your nose insist on being seen by a “Nose Specialist.” Failure to do so may have severe and inappropriate consequences for you. |